 Daniela Pinter1,2*
Daniela Pinter1,2* Simon Fandler-Höfler2
Simon Fandler-Höfler2 Viktoria Fruhwirth1,2
Viktoria Fruhwirth1,2 Lisa Berger1,2Gerhard Bachmaier3Susanna Horner2Sebastian Eppinger2
Lisa Berger1,2Gerhard Bachmaier3Susanna Horner2Sebastian Eppinger2 Markus Kneihsl2
Markus Kneihsl2 Christian Enzinger1,2,4
Christian Enzinger1,2,4 Thomas Gattringer2,4
Thomas Gattringer2,4- 1Department of Neurology, Research Unit for Neuronal Plasticity and Repair, Medical University of Graz, Graz, Austria
- 2Department of Neurology, Medical University of Graz, Graz, Austria
- 3Institute for Medical Informatics, Statistics and Documentation, Medical University of Graz, Graz, Austria
- 4Division of Neuroradiology, Department of Radiology, Vascular and Interventional Radiology, Medical University of Graz, Graz, Austria
Background: Patient-reported quality of life (QoL) may help to capture sequela of stroke more comprehensively. We aimed to investigate QoL in working age persons with ischemic stroke regarding impaired domains and identify factors associated with better QoL.
Methods: We invited persons with stroke aged 18–55 years to participate in this prospective observational study. We assessed QoL and self-rated health using the EuroQol 5 Dimension questionnaire (EQ-5D) during hospital stay (baseline) and at 3-months follow-up (FU). Additionally, the National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), cognition (Montreal Cognitive assessment, MOCA), emotion (Hospital Anxiety and Depression Scale), and return to work were evaluated. We used hierarchical regression to identify predictors of QoL (self-rated health and QoL Index score) at FU.
Results: We included 138 persons with stroke (mean age = 43.6 ± 10 years; 41% female; median admission NIHSS = 2), of whom 99 participated at FU. QoL Index and self-rated health were correlated with NIHSS, mRS, anxiety, and depression at both timepoints. Although 80% had favorable functional outcome at FU (mRS < 2), high proportions of these persons reported problems in the “Pain and/or Discomfort” (25.3%) and “Anxiety/Depression” (22.8%) dimensions. Only discharge NIHSS and baseline MOCA independently predicted self-rated health at FU. Female sex, higher discharge NIHSS, and higher baseline depression scores predicted worse QoL Index scores at FU.
Conclusions: Three months post-stroke, working age persons with stroke frequently reported problems in dimensions not assessed by the routinely used mRS. Despite correlations between clinical scales and QoL, patient-reported outcomes and screening for cognition and emotion ensure a more comprehensive assessment of post-stroke consequences relevant for QoL.
Introduction
Stroke at working age is on the rise, with ~10–15% of all ischemic strokes occurring in persons aged below 55 years (1, 2). These stroke survivors may live many years with detrimental effects in multiple health domains, such as physical, psychological, and/or social problems (3).
Some so-called “hidden” consequences of stroke (e.g., cognitive impairment, anxiety, depression) are not captured by routine clinical scales like the modified Rankin Scale (mRS) (4–6). Therefore, assessment of patient-reported outcome measures are increasingly recommended (7) to better capture diverse sequelae of stroke (5, 8).
To date, few studies have examined health-related quality of life (QoL) in working age persons with stroke (9, 10). Identification of factors influencing QoL in this patient group is essential to guide comprehensive clinical assessment and rehabilitation decisions and enable a more efficient and patient orientated (post-stroke) health care.
Prior studies highlighted physical impairment and psychological factors, such as depression, anxiety or fatigue to be associated with QoL in working age persons with stroke (11, 12). Recent work showed that in older persons with stroke, depression and cognitive impairment are independent predictors of participation and independence (13).
In this prospective, observational, and single-center analysis, we aimed to (1) assess patient-reported QoL and associated factors in working age persons with acute ischemic stroke and (2) identify potential predictors of QoL at 3 months post-stroke.
Methods
Participants
In this prospective, observational, cohort study, we invited all persons aged 18–55 years with an acute imaging-proven stroke (either ischemic or hemorrhagic) or cerebral sinus venous thrombosis from the Department of Neurology of the University Clinic Graz to participate in the Graz Stroke in the Young Study (February 2016-August 2020; N = 417) (14). The study protocol is shown in the Supplementary Materials.
The study was approved by the ethics committee of the Medical University of Graz. All participants gave written informed consent.
Health-Related Quality of Life Assessment
We assessed health-related QoL at the acute stage (during initial hospital stay in a clinically stable phase) and at 3 months post-stroke (follow-up, FU) using the EuroQol 5 Dimension - 3 level questionnaire (EQ-5D-3L) (15). The EQ-5D comprises five dimensions (“Mobility,” “Selfcare,” “Usual Activities,” “Pain/Discomfort,” and “Anxiety/Depression”) and three levels (“no problems,” “some problems,” and “severe problems”). We calculated validated index values (QoL Utility Index) from these severity levels, with higher values indicating better QoL (1 being best health state). Given that a representative validated Austrian QoL Utility Index is not available, we used the European Utility Index mean value derived from six countries (Germany, Netherlands, France, Spain, UK, and Denmark) (16). Furthermore, the visual analog scale (EQ VAS) recording persons' self-rated health on a scale ranging from 100 (“best imagined health”) to 0 (“worst imagined health”) was applied (15).
Clinical and Neuropsychological Assessment
All participants underwent routine neurological examinations and neuropsychological assessments during the initial hospital stay and at a pre-specified FU at 3 months post-stroke.
All but 11 participants undergoing cerebral CT underwent brain MRI. Neurological symptoms, vascular risk factors, stroke severity [National Institutes of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS)], stroke etiology (TOAST criteria) (17), and the affected cerebrovascular territories were assessed in every person. The mRS was evaluated by a trained mRS assessor. Cognitive function was screened using the Montreal Cognitive Assessment (MoCA), while Depression and anxiety were assessed with the Hospital Anxiety and Depression Scale (HADS).
For employed persons with stroke, return to work at FU, duration of sick leave within 3 months post-stroke (days), and self-reported impairment of employment (scale 0 “no impairment”−10 “severe impairment” at work due to stroke) were assessed.
Statistical Analysis
Demographic, clinical, neuropsychological, and QoL data was analyzed with the Statistical Package of Social Science (SPSS, Version 26). The Shapiro Wilk test was used to assess the normality of data distribution. We performed complete case analysis. We applied Wilcoxon test (for non-normally distributed variables) or paired t-tests. We used Spearman correlations to identify associations between QoL and demographics, and clinical and neuropsychological data. We performed two stepwise hierarchical regression models, including demographics (step 1), clinical (NIHSS and mRS at discharge; step 2), and neuropsychological measures (step 3) to identify potential predictors of QoL at FU (EQ self-rated health and Utility Index; Bonferroni-adjusted level of significance: 0.025).
Results
Patients
From February 2016 to August 2020, 168 persons with stroke were not able or did not want to participate. From the 249 participating persons, self-reported QoL assessment was available for 196 persons. Given the small sample size of other stroke subtypes and comparability with previous studies (11, 12), we focused on persons suffering from ischemic stroke [n = 138 (70%)]. Recruitment details, including a flowchart, are shown in Figure 1.
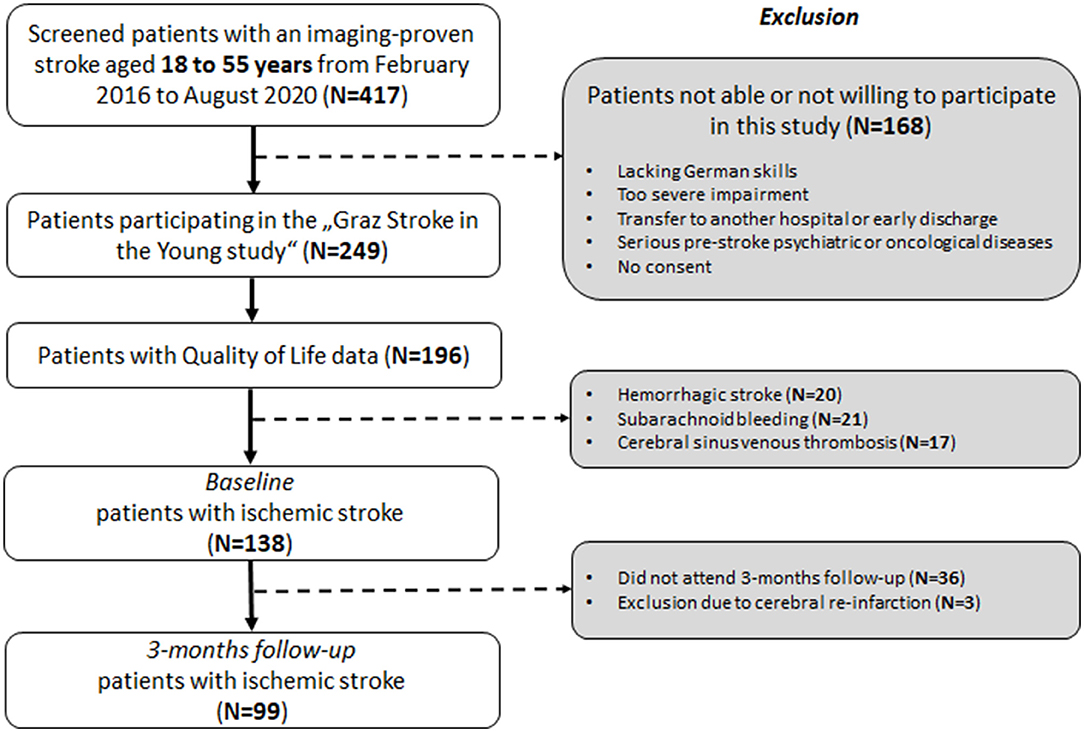
Figure 1. Flowchart of patient selection.
Regarding baseline (BL) characteristics (Supplementary Table 1), persons participating at FU (N = 99) did not differ from those who did not (N = 39).
Demographics and clinical and neuroimaging characteristics of the investigated ischemic stroke cohort are presented in Table 1. At baseline, data of 138 persons with stroke (mean age = 43.6 ± 10 years) was available (Figure 1).
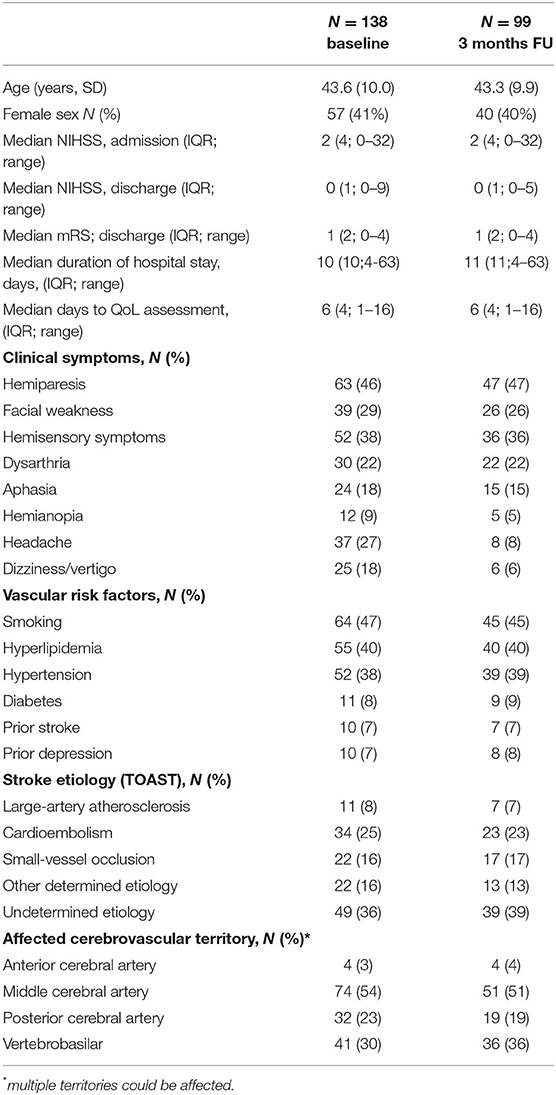
Table 1. Demographics and clinical and MRI characteristics for the cohort at baseline (BL) (N = 138) and for those with available follow-up (FU) at 3 months (N = 99) after ischemic stroke.
Sixteen persons (12%) received intravenous thrombolysis, 12 (9%) underwent mechanical thrombectomy, and 9 (7%) received both recanalization therapies.
QoL assessment was mostly performed on day 6 during hospital stay (Table 1). Neuropsychological scores at BL and FU are presented in Supplementary Table 2.
QOL at Baseline
At BL, 41.3% of persons with stroke reported serious problems in the domain “Usual Activities,” followed by 32.6% with problems in “Mobility,” and 31.9% reporting “Pain and/or Discomfort” (Figure 2A), while 39.9% reported no problem in any domain.
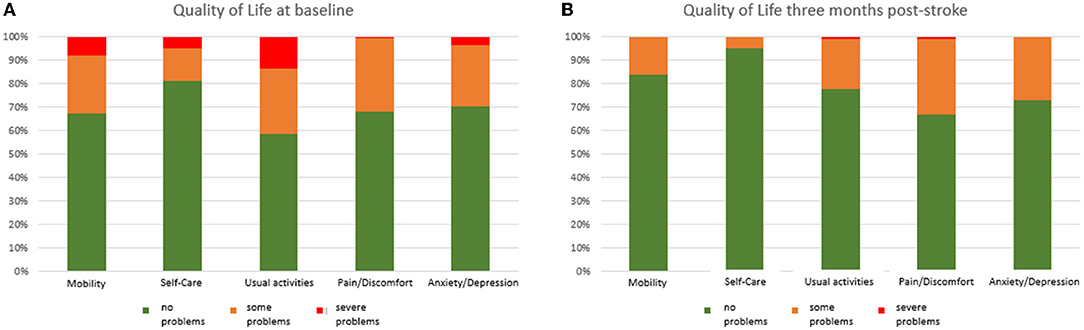
Figure 2. Proportion of problems for each domain at baseline [BL,(A)] and follow-up [FU,(B)].
Median self-rated health (EQ VAS) was 72.5 (IQR = 36.25; range = 0–100) and median QoL Index 0.89 (IQR = 0.34; range = 0.29–1).
Women reported a lower QoL Index compared to men (0.84 ± 0.34 vs.0.91 ± 0.28; p = 0.046). Age did not correlate with BL self-rated health or QoL Index. Persons with stroke of undetermined etiology (36%) did not differ from those with known stroke etiology in self-rated health (p = 0.433) or QoL Index (p = 0.715). Persons with diabetes indicated lower QoL Index (p = 0.004; Bonferroni-adjusted level of significance: 0.0083). No further clinical symptoms or vascular risk factors were associated with any QoL measure.
Self-rated health and QoL Index correlated strongly with clinical scores (r > 0.5) and moderately with HADS at BL and FU (r > 0.3) (Table 2).
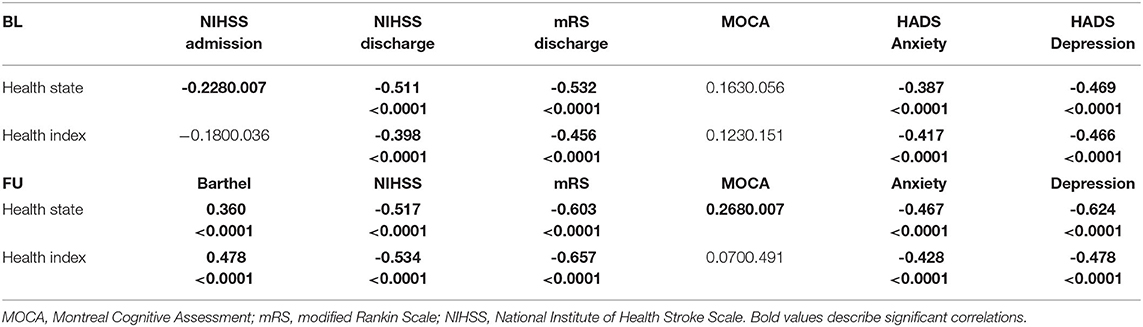
Table 2. Correlations between health-state and health index and clinical, cognitive, and emotional scores at BL and at 3 months FU.
QOL at 3 Months Post-stroke
The proportion of persons with serious problems at 3 months post-stroke was 33.3% for the Dimension “Pain/Discomfort,” 27.3% for “Anxiety/Depression,” followed by 22.2% for “Usual Activities” (Figure 2B), while 48.5% reported no problem in any domain.
Three months post-stroke, median self-rated health (EQ VAS) was 80 (IQR = 20; range, 30–100) and Median QoL Index 0.93 (IQR = 0.20; range = 0.41–1). Both measures were strongly correlated (rs = 0.633; p < 0.001). Notably, within the group of 79 persons (80%) with mRS scores of 0 (no symptoms) or 1 (no significant disability), 20 persons (25.3%) indicated problems in “Usual Activities,” 18 persons (22.8%) reported some problems in “Anxiety/Depression,” 9 persons (11.4%) reported “Pain/Discomfort,” 5 persons (6.3%) reported some problems in “Mobility,” and one person (1.3%) indicated some problems in “Self-Care.”
Quality of life 3 months post-stroke (self-rated health and QoL Index) did not differ with regard to sex or age, but correlated strongly with clinical scores, followed by strong and moderate (r > 0.3) correlations with HADS, and small to moderate (r > 0.1) correlations with MOCA scores at FU (Table 2).
Persons with prior depression indicated lower QoL Index values at FU (p = 0.001; Bonferroni-adjusted level of significance: 0.0083). No further clinical symptoms or vascular risk factors were significantly associated with any QoL measure.
Out of all initially working persons (N = 89; 90%), those who did not return to work (N = 48) within 3 months post-stroke reported lower QoL [self-rated health: 75 ± 30 vs. 90 ± 14.5; p = 0.002; QoL Index: 0.89 (0.25) vs. 1 (0.07), p < 0.0001]. Duration of sick leave correlated with self-rated health (rs = −0.375, p < 0.0001) and QoL Index (rs = −0.401, p < 0.0001) at FU. Self-reported impairment at work was strongly associated with self-rated health (rs = −0.587, p < 0.0001) and QoL Index (rs = −0.553, p < 0.0001).
Predictors of QOL 3 Months Post-stroke
Regarding correlations between baseline scores and QoL at FU, BL mRS and NIHSS correlated with self-rated health (rs = −0.442, p < 0.001/rs = −0.448, p < 0.001) and Qol Index at FU (rs = −0.573, p < 0.001/rs = −0.492, p = 0.034).
Baseline MOCA scores correlated with self-rated health (rs = 0.374, p < 0.001) and QoL Index at FU (rs = 0.214, p = 0.034). Baseline anxiety scores correlated with self-rated health (rs = −0.307, p = 0.002) and Qol Index at FU (rs = −0.320, p = 0.001). Baseline depression scores correlated with self-rated health (rs = −0.358; p < 0.001) and Qol Index at FU (rs = −0.357; p < 0.001).
In multivariable analysis, patient-reported self-rated health 3 months post-stroke was predicted by NIHSS at discharge (R2 = 20.7%; standardized beta = −0.377; p < 0.0001) and baseline MOCA score (incremental R2 = 11.2; standardized beta = 0.357, p = 0.001). Together, these showed a variance of 31.9%.
Patient reported QoL Index at FU was predicted by sex (worse for women, R2 = 5.6%; standardized beta = −.262, p = 0.007), NIHSS at discharge (incremental R2 = 25.5%; standardized beta = −.406; p < .0001) and HADS Depression score (incremental R2 = 4.5%; standardized beta = −.251; p = 0.017). Together these showed a variance of 35.6%.
Discussion
Our findings underline the importance of using patient-reported outcome measures to better capture the diverse sequelae post-stroke. Despite strong associations between routine clinical stroke outcome scores, such as the NIHSS and mRS, and QoL, approximately one-fourth of persons with no significant disability (mRS 0 or 1) indicated some problems in the dimensions “Pain/Discomfort,” and about one-fifth indicated problems in the dimension “Anxiety/Depression” at 3 months post-stroke.
Stroke-induced pain includes a heterogeneous group of conditions, such as pain due to spasticity, headache, and central post-stroke pain (CPSP) (18). In 5.9% of 824 working-age stroke survivors of the Helsinki Young Stroke Registry, persistent CPSP was observed and linked to lower QoL (18). Interestingly, we noticed that persons exclusively reported pain from headache at 3 months post-stroke (Table 1), but, notably, no one had CPSP. This could be explained by our less severely affected stroke population. Post-stroke headache associated with ischemic stroke is poorly understood, only occurring in ~14% of patients (19, 20). This underscores the importance to further explore headache associated with ischemic stroke to inform patient management.
Six persons indicating problems in the domain “Pain/Discomfort” reported to suffer from dizziness or vertigo at FU. Both are common post-stroke, and its multifactorial cause (e.g., visual impairment, sensory impairment, muscle weakness, illusion of movement) makes diagnosis and management challenging (21, 22).
Besides problems in “Pain/Discomfort,” relevant problems in “Anxiety/Depression” were reported 3 months post-stroke. It is noteworthy that according to the HADS, 18% of patients reported mild anxiety and 10% reported mild depression at FU, with only one person reporting to have severe anxiety and depression (scores > 15). Nevertheless, like in our study, working age stroke survivors frequently report feeling anxious, worried, less happy, and slowed down, affecting QoL (6). Due to the independent detrimental effect on stroke outcome, screening for mild depression and anxiety is thus increasingly recommended (6, 11, 23, 24).
Especially for persons clinically classified with an mRS of 0 or 1, assessing self-reported problems in mental health, cognition, and participation seem crucial to truly capture the multidimensional burden post-stroke (6).
In line with a study investigating older persons with stroke (13), both cognition and emotional factors independently contributed to the prediction of QoL and self-rated health at FU from NIHSS. Problems regarding cognition and emotion are highly prevalent in stroke, but receive little attention in clinical practice (25). In older stroke populations, cognitive impairment post-stroke has been shown to be associated with a range of worse outcomes (e.g., worse QoL, less independence, increased likelihood of depression) (26).
Screening all persons with stroke for possible cognitive impairment (e.g., Mini-Mental State Examination or MOCA) or increased emotional burden (e.g., HADS, or patient-reported outcomes, such as the EQ-5D) should be part of the standardized stroke assessment. Early identification and treatment of depression and cognitive impairment may potentially improve QoL among persons with stroke (12).
We found that the female sex was predictive of lower QoL Index scores at FU. A recent study investigating underlying reasons for poorer QoL in women post-stroke identified women's advanced age, more severe strokes, pre-stroke dependency, and post-stroke depression accounting for these sex differences (27). Reasons for lower QoL in working age female patients might differ, considering that women did not differ regarding age (p = 0.766), stroke severity (NIHSS; p = 0.690), or post-stroke depression (p = 0.892) in our sample. This needs to be explored further incorporating socioeconomic aspects in more detail.
Several post-stroke consequences are complexly inter-related. More severe functional impairments might result in higher dependency regarding activities of daily living, potentially leading to more severe depression or less participation. Conversely, more severe depression might lead to less participation, decreased performance in activities of daily living, or rehabilitation engagement. Many of these factors have been shown to influence the likelihood of returning to work, either in combination or independently (28).
In our cohort, persons not returning to work within 3 months post-stroke reported lower QoL. For those working, self-reported impairment at work was strongly associated with lower QoL. Interdisciplinary rehabilitation, including physiotherapeutic and psychological treatment, increases the ability to return to work post-stroke and, consequently, improves QoL (28–30).
The inclusion of patient-reported outcomes would not only help to more comprehensively capture stroke outcome (4), but is also recently shown to provide efficiency gains in stroke trials given the use of a “utility weighted mRS” (combining mRS and EQ-5D), leading to reduced sample sizes to detect treatment effects (31).
Several limitations have to be considered when interpreting the results of our study. Firstly, we did not assess fatigue, which was previously found to be associated with QoL post-stroke in working age patients (11, 12). Fatigue and depression are common consequences of stroke and are often inter-related. Both stroke-related symptoms interfere with the rehabilitation process and reduces QoL (32, 33). Secondly, the 3-month FU period might have been too short to adequately assess more long-lasting post-stroke consequences in daily living. Thirdly, we did not assess QoL in age and sex-matched healthy controls over 3 months. However, in addition to self-rated health, we calculated the European Utility Index mean value derived from six countries, which is a well-validated score to assess health-related QoL in clinical populations.
In conclusion, our data suggests that routine assessment of patient-reported outcomes may usefully aid to better capture comprehensive information on post-stroke consequences. The EQ 5D assesses subjective post-stroke problems in <5 min. In addition, such additional screening for cognitive and emotional problems seems promising to optimize individual treatment plans.
Data Availability Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University of Graz. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
DP, SF-H, CE, and TG contributed to the study conception and design. DP, VF, LB, GB, SH, SE, MK, and CE performed material preparation and data collection. DP performed data analysis. The first draft of the manuscript was written by DP and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.869550/full#supplementary-material
References
1. Ekker MS, Verhoeven JI, Vaartjes I, van Nieuwenhuizen KM, Klijn CJM, de Leeuw F-E. Stroke incidence in young adults according to age, subtype, sex, and time trends. Neurology. (2019) 92:e2444–54. doi: 10.1212/WNL.0000000000007533
2. Béjot Y, Delpont B, Giroud M. Rising stroke incidence in young adults: more epidemiological evidence, more questions to be answered. J Am Heart Assoc. (2016) 5:1–3. doi: 10.1161/JAHA.116.003661
3. Walters R, Collier JM, Braighi Carvalho L, Langhorne P, Katijjahbe MA, Tan D, et al. Exploring post acute rehabilitation service use and outcomes for working age stroke survivors (≤ 65 years) in Australia, UK and South East Asia: data from the international AVERT trial. BMJ Open. (2020) 10:e035850. doi: 10.1136/bmjopen-2019-035850
4. Deb-Chatterji M, Konnopka A, Flottmann F, Leischner H, Fiehler J, Gerloff C, et al. Patient-reported, health-related, quality of life after stroke thrombectomy in clinical practice. Neurology. (2020) 95:e1724–32. doi: 10.1212/WNL.0000000000010356
5. Rimmele DL, Lebherz L, Frese M, Appelbohm H, Bartz HJ, Kriston L, et al. Health-related quality of life 90 days after stroke assessed by the international consortium for health outcome measurement standard set. Eur J Neurol. (2020) 27:2508–16. doi: 10.1111/ene.14479
6. Rethnam V, Bernhardt J, Johns H, Hayward KS, Collier JM, Ellery F, et al. Look closer: the multidimensional patterns of post-stroke burden behind the modified rankin scale. Int J Stroke. (2020) 16:1-9. doi: 10.1177/1747493020951941
7. Quinn TJ, Paolucci S, Sunnerhagen KS, Sivenius J, Walker MF, Toni D, et al. Evidence-based stroke r-ehabilitation: an expanded guidance document from the european stroke organisation (ESO) guidelines for management of ischaemic stroke and transient ischaemic attack 2008. J Rehabil Med. (2009) 41:99–111. doi: 10.2340/16501977-0301
8. Reeves M, Lisabeth L, Williams L, Katzan I, Kapral M, Deutsch A, et al. Patient-reported outcome measures (PROMs) for acute stroke: rationale, methods and future directions. Stroke. (2018) 49:1549–56. doi: 10.1161/STROKEAHA.117.018912
9. Bartholomé L, Winter Y. Quality of life and resilience of patients with juvenile stroke: a systematic review. J Stroke Cerebrovasc Dis. (2020) 29:105129. doi: 10.1016/j.jstrokecerebrovasdis.2020.105129
10. de Bruijn M, Synhaeve NE, van Rijsbergen MWA, de Leeuw F-E, Jansen BPW, de Kort PLM. Long-term cognitive outcome of ischaemic stroke in young adults. Cerebrovasc Dis. (2014) 37:376–81. doi: 10.1159/000362592
11. de Bruijn MAAM, Synhaeve NE, van Rijsbergen MWA, de Leeuw F-E, Mark RE, Jansen BPW, et al. Quality of life after young ischemic stroke of mild severity is mainly influenced by psychological factors. J Stroke Cerebrovasc Dis. (2015) 24:2183–8. doi: 10.1016/j.jstrokecerebrovasdis.2015.04.040
12. Naess H, Waje-Andreassen U, Thomassen L, Nyland H, Myhr KM. Health-related quality of life among young adults with ischemic stroke on long-term follow-up. Stroke. (2006) 37:1232–6. doi: 10.1161/01.STR.0000217652.42273.02
13. Kapoor A, Lanctot KL, Bayley M, Herrmann N, Murray BJ, Swartz RH. Screening for post-stroke depression and cognitive impairment at baseline predicts long-term patient-centered outcomes after stroke. J Geriatr Psychiatry Neurol. (2019) 32:40–8. doi: 10.1177/0891988718819859
14. Pinter D, Enzinger C, Gattringer T, Eppinger S, Niederkorn K, Horner S, et al. Prevalence and short-term changes of cognitive dysfunction in young ischaemic stroke patients. Eur J Neurol. (2019) 26:727–32. doi: 10.1111/ene.13879
15. Szende A, Janssen B, Cabasés J. Self-Reported Population Health: An International Perspective Based on EQ-5D. Dordrecht Heidelberg New York London: Springer (2014). p. 1–196. doi: 10.1007/978-94-007-7596-1
16. Van Hout B, Janssen MF, Feng YS, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Heal. (2012) 15:708–15. doi: 10.1016/j.jval.2012.02.008
17. Goldstein LB, Jones MR, Matchar DB, Edwards LJ, Hoff J, Chilukuri V, et al. Improving the reliability of stroke subgroup classification using the trial of ORG 10172 in acute stroke treatment (TOAST) criteria. Stroke. (2001) 32:1091–8. doi: 10.1161/01.STR.32.5.1091
18. Harno H, Haapaniemi E, Putaala J, Haanpää M, Mäkelä JP, Kalso E, et al. Central poststroke pain in young ischemic stroke survivors in the helsinki young stroke registry. Neurology. (2014) 83:1147–54. doi: 10.1212/WNL.0000000000000818
19. Carvalho Dias M, Martins T, Basílio G, Lucas Neto L, Caeiro L, Ferro JM, et al. Headache at the chronic stage of ischemic stroke. Headache. (2020) 60:607–14. doi: 10.1111/head.13761
20. Harriott AM, Karakaya F, Ayata C. Headache after ischemic stroke: a systematic review and meta-analysis. Neurology. (2020) 94:e75–86. doi: 10.1212/WNL.0000000000008591
21. Ekvall Hansson E, Pessah-Rasmussen H, Bring A, Vahlberg B, Persson L. Vestibular rehabilitation for persons with stroke and concomitant dizziness - a pilot study. Pilot Feasibility Stud. (2020) 6:1–7. doi: 10.1186/s40814-020-00690-2
22. Kaski D. Neurological update: dizziness. J Neurol. (2020) 267:1864–9. doi: 10.1007/s00415-020-09748-w
23. Lee EH, Kim JW, Kang HJ, Kim SW, Kim JT, Park MS, et al. Association between anxiety and functional outcomes in patients with stroke: a 1-year longitudinal study. Psychiatry Investig. (2019) 16:919–25. doi: 10.30773/pi.2019.0188
24. Blöchl M, Meissner S, Nestler S. Does depression after stroke negatively influence physical disability? a systematic review and meta-analysis of longitudinal studies. J Affect Disord. (2019) 247:45–56. doi: 10.1016/j.jad.2018.12.082
25. Quinn TJ, Elliott E, Langhorne P. Cognitive and mood assessment tools for use in stroke. Stroke. (2018) 49:483–90. doi: 10.1161/STROKEAHA.117.016994
26. Rohde D, Gaynor E, Large M, Mellon L, Hall P, Brewer L, et al. The impact of cognitive impairment on poststroke outcomes: a 5-year follow-up. J Geriatr Psychiatry Neurol. (2019) 32:275–81. doi: 10.1177/0891988719853044
27. Phan HT, Blizzard CL, Reeves MJ, Thrift AG, Cadilhac DA, Sturm J, et al. Sex differences in long-term quality of life among survivors after stroke in the instruct. Stroke. (2019) 50:2299–306. doi: 10.1161/STROKEAHA.118.024437
28. Edwards JD, Kapoor A, Linkewich E, Swartz RH. Return to work after young stroke: a systematic review. Int J Stroke. (2018) 13:243–56. doi: 10.1177/1747493017743059
29. Westerlind E, Persson HC, Sunnerhagen KS. Return to work after a stroke in working age persons; a six-year follow up. PLoS ONE. (2017) 12:1–14. doi: 10.1371/journal.pone.0169759
30. Neau J, Ingrand P, Mouille-Brachet C, Rosier M, Couderg C, Alvarez A, et al. Functional recovery and social outcome after cerebral infarction in young adults. Cerebrovasculair Dis. (1998) 8:296–302. doi: 10.1159/000015869
31. Wang X, Moullaali TJ, Li Q, Berge E, Robinson TG, Lindley R, et al. Utility-weighted modified rankin scale scores for the assessment of stroke outcome: pooled analysis of 20 000+ patients. Stroke. (2020) 51:2411–7. doi: 10.1161/STROKEAHA.119.028523
32. Wen H, Weymann KB, Wood L, Wang QM. Inflammatory signaling in post-stroke fatigue and depression. Eur Neurol. (2019) 80:138–48. doi: 10.1159/000494988
Keywords: quality of life, cognition, emotion, working-age, stroke
Citation: Pinter D, Fandler-Höfler S, Fruhwirth V, Berger L, Bachmaier G, Horner S, Eppinger S, Kneihsl M, Enzinger C and Gattringer T (2022) Relevance of Cognition and Emotion for Patient-Reported Quality of Life After Stroke in Working Age: An Observational Cohort Study. Front. Neurol. 13:869550. doi: 10.3389/fneur.2022.869550
Received: 04 February 2022; Accepted: 14 March 2022;
Published: 25 April 2022.
Edited by:
Nishant K. Mishra, Yale University, United StatesReviewed by:
Birgitta Langhammer, Oslo Metropolitan University, NorwayMyzoon Ali, University of Glasgow, United Kingdom
Copyright © 2022 Pinter, Fandler-Höfler, Fruhwirth, Berger, Bachmaier, Horner, Eppinger, Kneihsl, Enzinger and Gattringer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniela Pinter, daniela.pinter@medunigraz.at